

Covid deaths in early 2020 and the use of Midazolam

I want to start by making two points:
Firstly, this post is about deaths. This isn’t an abstract concept – there were real people who were alive one day and dead the next. I knew some people who died during the Covid waves in 2020 and 2021, including one very good friend, and I miss them all. I ask that readers try to bear this in mind when thinking about the concepts that I’ll explore in this post.
Secondly, I must apologise to those who lost loved ones during the Covid waves in 2020 and 2021, because this post won’t help them in their grief. Nothing that is said now will bring them back, but it could bring back harsh memories that were best kept in the past, and introduce new uncertainties that will only make the grief worse. I’d very much have preferred to not have had to make this post, but it is important that we know what has happened so that we can learn from any mistakes that were made and try to ensure that they can’t be made again in the future.
Recently there have been a few posts on the topic of the use of midazolam and morphine to hasten death during the Covid waves in spring 2020 and winter 2020-2021. Most notable are the videos made by Dr John Campbell:
and
and the posts of Professor Norman Fenton:

These all reference a document produced by the National Institute for Health and Care Excellence, NICE, regarding treatment for those suffering from Covid, and which included a section on treatment for those near the end of life. This end-of-life care centred around the use of morphine and midazolam to ease the suffering of these individuals (as well as potentially other drugs; haloperidol and lorazepam).
The question that is now being asked is whether this end-of-life treatment might have been used too hastily, resulting in the death of individuals who might otherwise have survived. It is important to note that these guidelines came from NICE – this isn’t a simple guidance for medics, but a set of rules that they have to follow unless they have good reason to do otherwise.
Supporting this hypothesis is data on prescriptions for midazolam by GPs over the last few years:

Particularly of note is that pronounced peak in prescriptions written for Midazolam in April 2020, and a smaller peak in winter 2020-21.
Unfortunately, the graph of GP prescription data doesn’t tell the full story – there’s also the use of these drugs within a hospital environment. Data for hospital use of drugs is available here. I consider it a bit of a shame that these data are so awkward to use – almost as if the NHS were required to publish the data, but weren’t so interested in ensuring that the public could actually see what was going on. Nevertheless, it is possible to analyse these data to identify trends in hospital use of different drugs.
First there’s midazolam:
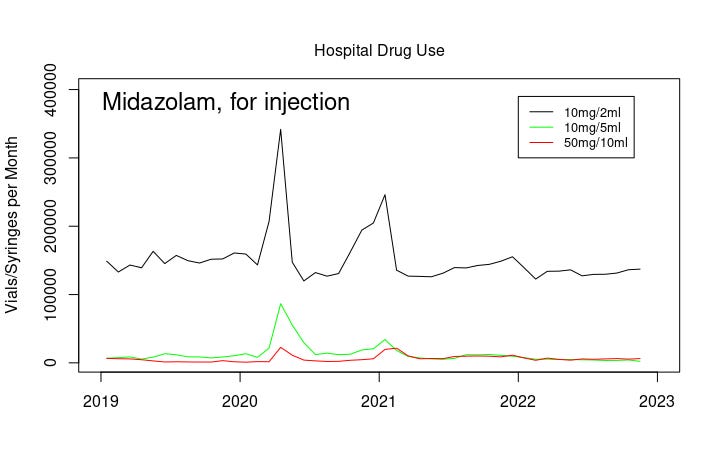
These data show that even in normal times hospitals use far more midazolam than GPs – compare the GPs 20,000 prescriptions per month with the near 150,000 vials per month just for the 10mg/2ml vials of midazolam. Note that they have good cause to use this drug – it is often used before surgery and other medical procedures to induce sleepiness and reduce anxiety at a time when the patient is probably, and quite reasonably, apprehensive about their upcoming procedure. NHS hospitals perform around a million surgical procedures per month, so the baseline use, while seemingly high, is in proportion to the medical need.
And, of course, note the huge peak in use in April 2020 and winter 2020-2021. For the 10mg/2ml preparation that’s more than twice the normal usage, at 200,000 additional vials in a single month.
There’s a similar pattern in the use of morphine in hospitals. First morphine for infusion (ie, introduced via a ‘drip’):

Note that morphine is also used in vials of 100mg/100ml and 250mg/250ml – these preparations are often used within hospitals but didn’t show a significant increase over this time period.
And in addition, morphine for injection:

Note that by far the most commonly used form of morphine is in vials of 10mg/1ml (at around 250,000 vials used per month this is far in excess of the quantities shown in the graph above), however there appears to have been no similar increase in use of this preparation of morphine over the time period in question.
Again, it is important to consider that morphine is used extensively within hospitals for the relief of severe pain, and the baseline levels (including in other preparations of morphine that didn’t show a significant rise during the times in question) are to be expected. It is also important to note that drugs that have been prescribed aren’t necessarily used – it could well have been that during April 2020 doctors ‘gathered resources’ in anticipation of a problem that didn’t materialise, at least to the apocalyptic levels forecast by government ‘experts’.
I’ll also reiterate – the use of morphine and midazolam presented above is in addition to the use of these drugs by GPs, as described in recent posts by others.
Thus it appears that there was also a significant rise in the use of certain preparations of midazolam and morphine within hospitals during April 2020 and winter 2020-2021.
But what does all this mean?
It might be tempting to reason that all of these vials of morphine and midazolam were used to kill people. I suspect that there are those who suggest that this approach might have been used deliberately to ‘clear beds’ in early 2020. It is certainly easy to forget that during spring 2020 we were all told that the hospitals would be overflowing with Covid patients and at that time the ‘Nightingale hospitals’ were starting to get constructed (never to be used). However, I think that this particular use is unlikely. Doctors aren’t evil people (with a few obvious exceptions) and wouldn’t go along with ‘orders from above’ to commit such atrocities. Furthermore, even if there were a few psychopaths amongst their numbers, there would have been other healthcare workers around them who would have picked up on any staff who were deliberately causing death in those who weren’t otherwise at their life’s end. That said, it cannot be assumed that healthcare professionals will self-police in this way – there are occasions where individuals work alone, and there is always the suspicion that there might be a certain amount of ‘closing-rank’ when criticism of behaviours is expressed (whether or not suspicions are reasonable).
At the opposite extreme, it is possible that all of these vials were used in a genuine act of kindness, easing the suffering (but not promoting death) of individuals who were very very ill with Covid and who were clearly in their final hours of life. It is important here to point out that medics see much more of life and death than many of us would care to see; in their career they will almost certainly have to make difficult decisions/recommendations on behalf of their patients, and it is surely a heavy burden to carry. In particular, front-line healthcare staff in 2020 and 2021 will have seen patients in respiratory distress, something that they will almost certainly have found distressing themselves and they would have looked for ways to relieve this distress in their patients. We certainly shouldn’t demonise medics when they have acted with compassion, nor their instruments where they were wielded with care.
However, I fear that there is a likelihood that we have had a ‘middle ground’ – the NICE guidelines appear to have introduced a pathway for doctors which allowed for (perhaps even encouraged) more than a gentle nudge for those who were ill with Covid towards death, some of whom might well have survived given the chance. This iatrogenesis hypothesis would mean that at least some of the deaths recorded as with Covid might well have been a direct result of the care guidelines as set out by NICE.
It is easy to forget now that we’re living with Covid that there was a great deal of fear of Covid back in early 2020 – the government official line was that Covid was a very serious disease in all and a near death-sentence for the vulnerable. Furthermore, all of the mainstream media had been co-opted to ensure that the entire population was constantly reminded of this (and had been induced into terror at the intended level) and to quash (and de-platform) any dissenting voices. This fear would naturally have affected our healthcare workers, and there is no doubt that there would have been reluctance to spend too much time with the infected, at least in those early days. What’s more, healthcare workers were instructed to limit time with the infected, to reduce the risk of themselves catching Covid or passing it on to other patients in hospital. This might have been made substantially worse by official messages of the very high case fatality rate of Covid in the early days of the pandemic – it would take a little time before healthcare workers would gain a practical understanding of the true lethality of Covid in the various vulnerable groups. Whether this fear might have altered the notion of what healthcare workers considered ethical is something which must be considered.
It is also important to consider the differences in approaches to care that you’d find in a major incident compared with normal times – healthcare workers would have been expected to expend their efforts in saving those who could be most readily saved, with those considered to have a lower chance of survival offered what support could be spared. Thus there is the likelihood that some decisions would have been made with what might now be considered insufficient patient contact to make a full assessment of the situation. This might be considered even more likely in situations where patient assessment was given over a video link or even after verbal communication with inexperienced nursing staff. In particular, there are questions to be asked of how this policy was communicated with with care-home staff, and what safeguards were put in place to ensure that the policy wasn’t poorly applied.
It is important to note that in the iatrogenesis hypothesis it isn’t necessary for some people to have had an evil intent – it is entirely possible that individuals promoted and exercised a policy that resulted in needless deaths while believing that they were ‘doing the right thing’ (eg, see Hannah Arendt’s concept of the banality of evil https://en.wikipedia.org/wiki/Eichmann_in_Jerusalem). In particular, ‘petty bureaucrats’ appear to be readily able to think up policies without seeing the need to consider the full consequences, and when these consequences are eventually revealed will usually point to the minutes from endless meetings with other petty bureaucrats to show that they weren’t personally responsible for the policy and they were simply following process. Of course, once a framework had been decided front-line staff might have been grateful for the guidance offered given the challenging times, at least until the negative consequences of the guidance became painfully clear.
The questions thus become: Who exactly was responsible for this approach to be taken for those seriously ill with Covid? Was there any ‘encouragement’ delivered from those in government? What happened to any feedback/criticism of the approach from front-line medical staff or from experts in medical ethics? How was the decision eventually reached to withdraw this guidance?
It is vitally important that we understand what has happened here, not only because if mistakes were made they should never be allowed to happen again, but also because we need to understand whether there should be safeguards in place that could have prevented any mistakes from happening in the first place. If there is a need to alter the power-relationship between guidance authorities (NHS ‘leadership’, NICE, MHRA, JCVI, etc) and medical staff then this needs to be undertaken as soon as possible. Similarly, if the mechanisms in place to allow healthcare workers to report inappropriate working practices aren’t working (or if they are working but no-one pays any attention in the end) then this needs to be rectified.
Note that the problem with healthcare in 2020 and 2021 is broader than the potential issue of midazolam and needless deaths – any investigation into healthcare during this time should certainly include community healthcare, the lack of GP provision and, particularly, the experiences of those in care homes.
Finally, we need to fully understand if the people who ‘encouraged’ this approach were actual medical personnel or if the ‘orders came from above’, made by civil servants with motives other than the well-being of those who placed their care in the hands of the NHS.
Note that this isn’t a trivial consideration, simply trying to find ‘the right people to blame’ for the mess that we’ve had over the last 3 years -- trust in our healthcare systems is a very important factor, something well understood over two thousand years ago and embodied in the Hippocratic oath. We’re already seeing the erosion of trust in traditional vaccines because of politicians’ declarations of ‘safe and effective’ for the Covid vaccines which have turned out to be rather complicated beasts. If medical professionals around the world don’t grasp the opportunity to have an open and honest conversation about the mistakes that were made we run the risk of forming a serious distrust in medicine in general.
I have written before about the need for a ‘truth and reconciliation’ approach to the official Covid response. Instead our leaders appear to favour the ‘stick it out’ approach, where they steadfastly refuse to acknowledge any deficiencies in the decisions made in 2020 and 2021. As far as they’re concerned Covid was a terrible disease that killed indiscriminately, lockdowns were necessary and saved lives, facemasks were necessary and saved lives and the safe and effective vaccines were necessary and saved lives. Unfortunately for them, science and medicine aren’t like economic theory – governments might be perfectly capable of making decisions on our countries economy without there being an easy way to ever prove that they were wrong, however, when it comes to science and medicine eventually the truth will out. I suggest that our authorities would be well advised to consider an open and transparent review of what occurred over those two years, with encouragement given to relevant scientists and medics to come forth and discuss their experiences during the pandemic.
I love the balance and nuance pf your article which is necessary, of course, because it is almost impossible to make any conclusive argument on intention. However, one thing, IMO, that is conclusive is that "centralisation" is the root problem. Our society has evolved into an incredibly lazy one that relies way too much on credentialism and authority. This laziness is not just the benefit club, lounging about on sofas at the expense of productive members of society, it is also the doctors you talk about. Yes, NICE is absolutely at fault if it is a set of legal guidelines that doctors should follow but is there not a mechanism for doctors to challenge NICE, no matter how long it takes? If not, that is exactly the problem, as always. Too much power concentrated in the hands of few doesn't need to be corrupted to yield sub-optimal outcomes. Decentralisation is the solution for public health and all the other failures of the current government system.
This is rearing is head a lot currently and I think there are major crossed wires. So to clarify I am a GP worked through the "pandemic" across 3 practices in the North West. At no point did I ever subscribe to the death rate, lockdown and am unjibbed.
Just to be clear I think there have been many,many catastrophic problems with how COVID was handled -failure to admit, inappropriate discharges , lack of access to service (or fear from patients taking up service), loneliness, failure to protect elderly by discharging positive cases into homes or with vulnerable spouses etc all contributed to deaths and are unacceptable -I do not wish in any way to defend these actions.
What I do not believe happened was lots of people were given midazolam early and inappropriately - I have many contacts around the country as you might imagine and have seen nothing to suggest this. What didhappen was that in March 2020 a concerted effort was made to look at patients in whom they had either already expressed wish never to be admitted to hospital or it was manifestly clear admission was not appropriate and their end of life care plans were updated. Alongside this just in case (JIC) drugs would be issued to be available -this includes midazolam and morphine. This is good practice and efficient GP practices would have mostly already have this covered but many would have found patients in whom this had not been done and caught up. To be clear this is what should happen to avoid suffering from delays contacting out of hours doctors and pharmacies to try and access drugs that should be available already.
Hence the spike in prescribing -I saw no evidence of increased usage. Can I say it never happened - no , do I think the issue re midazolam is however is largely explained by the above- absolutely yes.