

Concerning trends in the Hospital Consultant Data for the Post-Vaccination Period

The UK NHS supplies updates on the number of times each hospital consultant speciality is used within each month. This data set is rather large, and includes multiple specialities, from General Surgery to Sport and Exercise Medicine, and covers a variety of consultant responses, from Emergency Admissions to whether it is a follow-up appointment. Note that this isn’t all hospital activity, but it does indicate relative changes between hospital specialities over time.
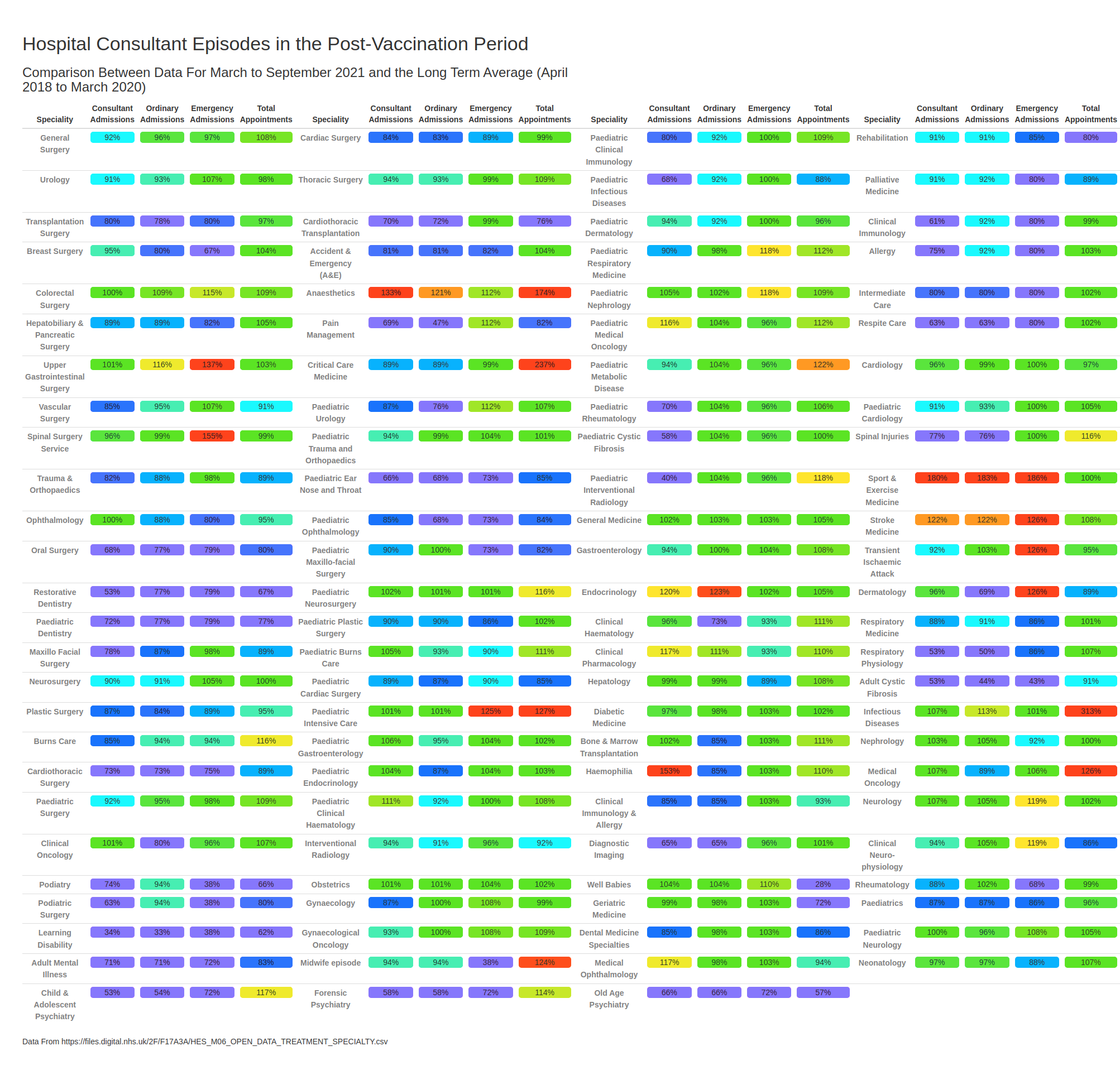
I’ve summarised a subset of this information in the table below. The data are presented as the percentage change in activity between the pre-covid era (up to March 2020) and the post-vaccination era (after March 2020 — note that data for January and February 2020 are not included for the post-vaccine period as there was a significant reduction in activity resulting from the winter lockdown in the UK).
To help visualise the changes, the table is colour-coded — greens for ‘not much change’, blues where there has been less activity than in the pre-covid era in recent months and reds for where there has been more activity than in the pre-covid era.
(Click on image for full-size version).
At a glance it can be seen that while there are many areas in which activity has returned to near normal levels (green) there are rather too many areas where activity is still running significantly below the historical rate (blue). I would suggest that while it is possible that people have suddenly become more healthy (eg, by covid killing all the unhealthy ones), it is far far more likely that the reduction in the activity for the ‘blue’ specialist areas is only due to the NHS reopening more slowly in those areas.
Anyway, today I want to concentrate on the red areas, which indicate that activity is higher than was historically the case, and to discuss why we might be seeing this increased hospital activity.
For some of these ‘red’ areas it is likely that the activity is mainly a result of covid itself — infectious diseases is clearly related, but anaesthetics and critical care will likely include a substantial number of those in intensive care.
But it is the others that concern me.
Stroke appears to be up over 20% compared with the long term average. I note that strokes can be caused both by blood clots (thrombosis, which has been identified as associated with the vaccines) and by bleeding (haemorrhage, which has also been identified as associated with the vaccines).
Transient Ischaemic Attack (aka ‘mini-stroke’) shows a substantial increase for emergency consultations.
Sports and Exercise Medicine has had a substantial increase in consultations compared with the pre-covid period. Surely this can’t all be due to very rare incidents of professional football players suffering from heart problems?
Emergency Upper Gastrointestinal Surgery shows a substantial increase. I note that there are high numbers of entries for ‘abdominal pain’ in the UK’s Yellow Card vaccine side effect database.
Emergency consultations regarding Spinal Surgery also shows a substantial increase. I don’t know why this should be — there’s no particular signal for back problems in the Yellow Card database. On the other hand, I know of rather a few people who are currently complaining of a bad back…
Paediatric Intensive Care consultations are up substantially.
Medical Oncology (cancer treatment without radiotherapy) total consultations are up substantially (26%). This is odd as Clinical Oncology (cancer with radiotherapy) consultations haven’t seen a similar increase.
There is also an increase in emergency consultations regarding Dermatology. This sounds like it can’t possibly be related to the vaccines or covid, but note that shingles and purpura might lead to a referral to a dermatology consultant. On the other hand, there might be a seasonal effect in these specific data.
Of course, we have had three big changes in our medical provision compared with the pre-covid era:
Covid itself. This clearly has some impacts on health beyond simply respiratory disease. I note, however, enormous efforts have been spent trying to identify longer term complications following infection with the Sars-Cov-2 virus and it is unlikely that any stones have been left unturned. I also note that it is possible that other diseases might influence health in a similar way (ie worst cold ever).
Lockdown. It is obvious that lockdowns have impacted on the ability of the healthcare system to fully respond to people’s needs, and that this might have had a visible impact on some medical areas. I’d suggest that this might be particularly noticeable in cancer rates, where people might have had delays in relevant testing, etc. I’d also suggest that other specialist areas would not be affected by lockdown in the longer term — for example, strokes require immediate medical attention and there is no option to delay for a few weeks because hospitals are busy.
The vaccines. The data shown in the table is for the post-vaccine period — are at least some of the substantial increases seen in specialist activity related to vaccine side effects?
The data shown in the table suggests that the vaccines might have introduced a risk of hospitalisation for some specialist areas. If only they would release these data by vaccination status so that we could investigate further… but, as I have noted previously, the authorities seem very reluctant to release any data that might show up a negative effect of the vaccines.
More work must immediately be undertaken in this area to fully understand the role of the vaccines in these changes and whether this would impact on the current aims to achieve full covid vaccination throughout the world.
Finally, I note that Cardiology appears to show no change between the post-vaccine era and the pre-covid era — in my next post I’ll explain why this is surprising.
If only, say, we still had a blinded arm of a decent sized original trial....
Another footballer with "chest pains" - https://www.mirror.co.uk/sport/football/news/adama-traore-sheriff-champions-league-25541132