

Enough about mortality -- what about morbidity? Some additional information.
The difficulty of working only with observational data

There’s no need to read this post. Really, there isn’t.
I’m going to be putting up some more posts about the UK data on hospital activity and use of medicines and it is likely that some people will say ‘ah, yes, but’. The aim of this post is to put some context on the data that I’ll be presenting, to preempt some of these criticisms. If you have questions about the data I’ll present in some of my later posts it is possible that I’ve covered it in this post — have a look here first, and if you’re not satisfied pop up a comment and I’ll try to answer.
Before I start reporting on evidence of other morbidities in the various UK NHS data sources, it is first necessary to check that we’ve not simply had the NHS suddenly become far far more efficient in 2021, with all hospital consultants working overtime to get the UK’s population back to rude health. In general, the NHS consultant activity data shows a return to normal workload levels, albeit with little ‘catch up’ for missed activity during 2020 being visible in the data – the data for consultations with ophthalmology experts (from the NHS hospital consultant activity data) is a good example:

That said, there are a few examples of specialist areas which haven’t returned to normal. For example, the consultations with experts in the lower leg and foot show a sustained reduction in activity:

I presume that individuals with medical problems with their lower leg / foot have are expected to be patient and that the NHS will get to them when it has time – after all, there is a climate emergency to worry about and the war in Ukraine has affected us all in complex ways.
It is also difficult to interpret data from drug prescriptions given by GPs in the UK – for example, prescriptions for antidepressants have increased in the last two years, but only in line with the general trend (which is depressing enough in itself):

Antidepressants (https://openprescribing.net/bnf/0403/)
Then there are associations with the Covid period that appear straightforward until you delve a little more into the situation. Take the issuance of prescriptions for famotidine:
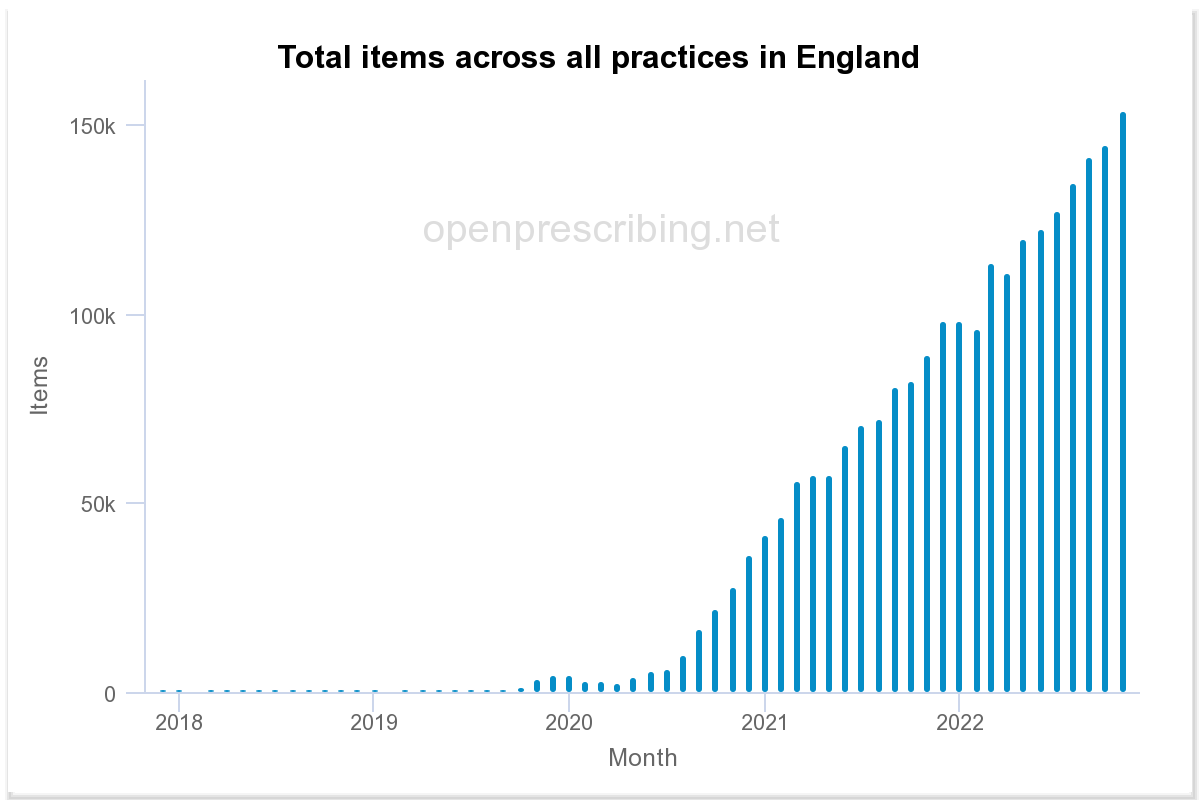
Prescriptions for Famotidine. From https://openprescribing.net/chemical/0103010H0/
Famotidine is a drug used to treat and prevent serious heartburn in individuals. On the face of it the above chart could be interpreted as evidence that Covid infection results in heartburn and that the vaccines only make this worse, however, further research finds Ranitidine, another heavily used drug used to treat heartburn, had its licence in the UK revoked in early 2020 due to contaminants being found in samples. Thus it is most likely that this significant increase in the use of Famotidine was simply due to it being a readily available alternative, but even if there was a link with Covid (this remains a possibility) this complication would result in these data being of little use in finding it. In my analysis of changes to NHS treatments in the Covid period I have tried to remove any statistical signal where there are similar ‘complications’ to the story.
Finally, there are those drugs where there is a potential statistical signal buried on top of another, larger, signal. Take prescriptions for ADHD drugs (eg, methylphenidate; usually known as ritalin or concerta) in the UK:

ADHD drugs (https://openprescribing.net/bnf/0404/)
A statistical analysis shows that there was a change in the increase in prescription of ADHD drugs around mid 2021, visible as a slight change in the gradient of the bar-chart. A quantitative analysis of these data shows that the rate of increase of prescriptions for ADHD drugs changed from around 1,000 new prescriptions every month in the pre-Covid era to nearly 2,500 additional prescriptions every month in the post-vaccine period. A statistical test of this change suggests it to be statistically significant. But what was the cause of the change – was it a case of Covid or the the vaccines producing ADHD? Was it the result of frustrated parents during our lockdowns? Was it just the continuation of the slow medicalisation of ‘slightly naughty children’ that we’ve seen over the decades coupled with GPs having less time available for face-to-face consultations? I really don’t know the answer to this – in the analyses that I’ll offer over the next few posts I’ve tried to restrict myself to only presenting data where I think there might be something truly significant going on, but this doesn’t mean that there aren’t more nasties hiding in the data.
In summary: The NHS hospitalisation data appears to show a strong statistical signal suggesting that there has been a significant increase in strokes in the UK population . Other data suggests that this isn’t due to a general ‘catching up’ being undertaken by the NHS, but is a real effect. In my next posts I’ll explore some other risk factors emerging from different sources of NHS data.
I'm sure you are right about famotidine. We spent years weaning people off PPIs and on to ranitidine, which was a long hard slog as PPIs are hopelessly difficult to wean off because of rebound acidity. Then ranitidine was taken off the market so all those people went back on PPIs. Now we have famotidine and we're starting back at square one. It is also used in Long Covid due to all the chat about mast cells n the long covid community, but I suspect that is a very small proportion of scripts overall. Also used for chronic urticaria which I have seen after Covid immunisation but can also be triggered by viruses. Mostly though it is used for reflux.