Enough about mortality -- what about morbidity? Part 2
It's in the blood

Before I start delving into the data, I should start with pointing out that it can be rather difficult to work with simple observational data. I recall back in 2021 having a series of online discussions with an individual about many aspects of the Covid vaccines, including the statistical analysis of data that has come purely from observations; I said that it was surprisingly difficult and that is pretty much why matched cohort randomised/blinded trials were undertaken in the first place, while they were adamant that it was easy and that there was thus no need for proper trials to be conducted. I didn’t mind these discussions in the slightest because that is how science works – through challenge and the need to explain your position through logical argument with reference to relevant understanding of the science, past experience and emerging data. I now realise that this individual (or series of individuals) was very likely a member of 77th Brigade trying to suppress anti-vaccine sentiment, however this doesn’t take away from the need to have scientific discussion and debate (but probably does explain their dual characteristic of being surprisingly well informed regarding immunology, yet being completely unable to comprehend anything that deviated from the government’s narrative, such as the concept of imperfect vaccines, vaccine driven viral evolution or the fact that vaccine side effects can take longer than 28 days to emerge). I now consider that those online discussions were a bit of an own-goal for 77th Brigade as they allowed a nice discussion to take place regarding the Covid vaccines and their potential flaws, exposing readers to a series of scientific and logical based rationale as to the risks of the mass vaccination programme, many of which have materialised – thanks 77th Brigade.
For want of a particular place to start, I’ll begin just about where I left off in my post about an apparent increased risk of stroke that emerged at the turn of 2020/2021, and my observation that emergency prescriptions for apixaban, a drug used to decrease the ability of the blood to form clots, had increased markedly in the last 24 months. An interesting observation is that in the past few months there has also been an increase in emergency prescriptions for tranexamic acid, a drug used to promote blood clotting:
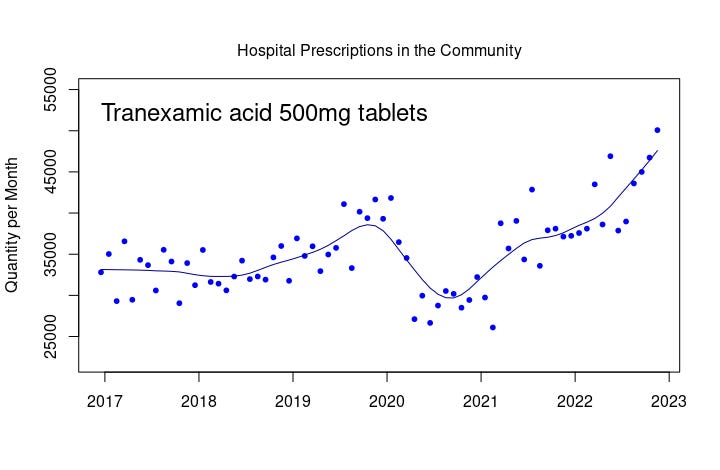
Tranexamic acid prescribed in hospital for dispensing in a normal pharmacy. Line is LOWESS smoothing with f=0.2
I consider the above to be a fascinating graph. In late 2019 something happens that increases the use of tranexamic acid – is this yet another indication of Covid being endemic in the UK in late 2019? The reduction in use in 2020 almost certainly simply aligns with the near shutdown of healthcare in the UK, with the surprise being a significant rise in the use of tranexamic acid above pre-2020 levels during 2022.
Since tranexamic acid is used to promote clotting, what about the most famous disease affecting blood clotting, haemophilia? This is an inherited disease where those affected will know of their condition and how best to manage it – yet for some reason in early 2021 there was a sudden rise in hospital admissions where the individual required an infusion of Factor VIII, the compound required by haemophiliacs (type A) to control their ability to form blood clots:

Factor VIII, hospital use. Line is LOWESS smoothing with f=0.2
At the same time, there was also a similar increase in activity of consultants specialising in haemophilia in UK hospitals. Sure, these are small numbers, but there are only about 20,000 people in the UK with either haemophilia or von Willebrand disease (a similar condition with reduced clotting ability in those affected), thus whatever happening in early 2021 will likely have affected a fairly large proportion of this section of our population.
Clots are used to prevent blood being lost from our arteries and veins, whether by wound, trauma or the natural leakiness of our blood vessels. Has there been any changes the ability of our blood to perform its job of transporting oxygen and nutrients around the body?
Anaemia is a condition where the blood becomes less capable of transporting oxygen (and not simply as an iron deficiency, which might be a common problem but isn’t the only cause of anaemia). The GP prescription data show a very slight increase in drugs associated with low iron, but more significant is the increase from the start of 2021 of the issuance of prescriptions for treating megaloblastic anaemia, which is related to problems with red blood cell production rather than simply iron levels in the blood:

Medication for megaloblastic anaemia (https://openprescribing.net/bnf/090102/)
At the same time, there has been an increase in the use of Folic acid, a drug used to stimulate the production of red blood cells, within NHS hospitals:

Quite why there should be a problem of low levels of red blood cells starting in early 2021 is unclear.
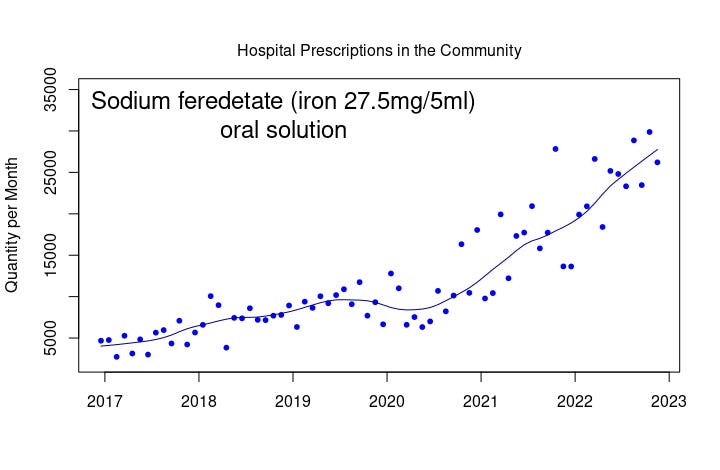
During 2021 there was also an increase of emergency prescriptions for sodium feredetate, used to offer increased iron to be used in the production of haemoglobin, the substance that ‘carries’ the oxygen within red blood cells:
And there’s even been a significant increase in the use of ferric derisomaltose, which is used when there is a clinical need for a rapid increase in iron and where the patient has not responded well to other forms of iron:

I must add that there doesn’t seem to be a visible increase from 2021 onwards in the numbers taking the more regular forms of supplemental iron, such as iron sulfate, within hospitals.
From normal people attending hospital with problems with clotting or anaemia, to individuals suffering from a rare inherited condition, we appear to have had strange goings-on in the nation’s blood. Is anyone going to investigate this aspect of our nation’s health?
It is worth mentioning that the hospitals and haemophilic data are for those individuals whose condition warranted hospitalisation – has there been a similar impact on individuals’ blood clotting that hasn’t been of sufficient magnitude to result in the seeking of medical care? We just don’t know – yet again, a proper investigation is warranted.
Oh, and what of my 77th Brigade friend? He still pops up from time to time, desperate to inform everyone about what they’re expected to think at that moment. Most recently it was that Covid had gone away and that everyone should forget about what had happened. I imagine that he’ll be along soon enough to tell everyone that we really shouldn’t be trying to punish those that used such oppressive techniques to suppress independent discussion on the topic of the official Covid response and the Covid vaccines.
This is super interesting. It suggests that there is an increasing in bleeding disorders starting abruptly in Jan 2021. The first candidate that comes to mind is aplastic anaemia. Tranexamic acid is also used for heavy menstrual bleeding which of course would only affect under 55s but would also cause anaemia.
The April 2020 figures are skewing your LOWESS function because they are artificially low due to hospital closures. Consider removing these points from the function and replot, you should then see when the take off in prescriptions was more clearly.
Thanks again, appreciate your work. I would love to know the attendance rates to Emergency Depts for miscarriage/threatened abortion and dysmenorrhea, as an ED doctor of over 25 year's experience I've anecdotally never known so many attendances for of these presentations.